Forum Replies Created
-
AuthorPosts
-
 Keith TaylorParticipant
Keith TaylorParticipant
I based my “no clue” opinion on recent posts to this convoluted thread, including responses to my view on allopurinol dosing at https://goutpal.net/forums/topic/question/#post-4625
I’m sorry if I’ve missed something, but I gained the impression that you were unhappy with your doctor randomly changing your dose from 100 to 300 without proper blood tests and a clear target.
Unfortunately, this is what happens in the casual gout help area compared with a structured help plan. Especially when we get at least 4 threads within a single topic (bunions, allopurinol dosing, gout footwear, and side effects). Because it is easy for me to miss salient points.
In any case, the only controversy for me is moving from 100 mg to 300 mg without professional scrutiny of blood test results for uric acid, kidney function, and liver function.
So, if you had that scrutiny, but I missed the point somewhere, I suggest you simply get on with the 300 mg dose. But, if you have questions about that, then start new topic(s).
On the other hand, you might still be wary of moving to 300 mg now. If so, please start a new topic on that subject.
Whichever is your best choice, please remember, there is never a “best way” to recover from gout. Only, the best way for you, or for any other individual gout patient. Which is why doctor’s struggle to deal with gout patient relationships. Because they never have enough time to discuss individual needs and preferences.
My struggle is slightly different. Because I need to learn about each GoutPal member’s unique history, aspirations, and current situation. Only when you teach me about those things can I give you the best personal help.
Let’s learn about your gout together.
Keith TaylorParticipantRebecca, there’s a wide choice of pill-splitters from Amazon, eBay, and similar outlets. But, if it were me, I would just take a pill on alternate days to get a half dose.
I must point out that won’t work with most prescription drugs. But the way allopurinol works, it ought to be effective. Normally, I’d suggest confirming this with your doctor. Which won’t work for you, as your doctor has no clue. Maybe you can talk to the pharmacist who supplied your allopurinol?
Keith TaylorParticipant“most comfortable orthopedic sandals with Velcro fastenings” sound good for gout. Especially the Velcro fastenings that I still insist on even with no gout pain. Because I got used to Velcro fastenings which helped me when I had painful feet. So, I still find them much more comfortable, and easier than laces.
Perhaps Rebecca, in your case, the orthopedic sandal is better than a stronger shoe or boot. In my case, I used to get quite a lot of ankle gout pain. So, a boot or stout shoe was best for me. But, your situation is different and you should listen to qualified physio or podiatrist. However, make sure that you mention that you need shoes to support gout-damaged feet as well as help with your bunions.
Keith TaylorParticipantThanks for reporting that poor quality page. Now, I’ll work on improving it as soon as I can.
Please, can I ask, if you spot any more of my mistakes that you post links to those pages as well. Because that will allow me to fix them quicker.
Thanks again nobody.
Keith TaylorParticipantHi Rebecca,
Firstly, I’m sorry I’m late to respond to you, but the depression hit me pretty hard recently and I (wrongly!) took to my bed. Anyway, my mate and I have come up with a plan to try and prevent recurrences. So, I hope to be more responsive to you in future.
I only mention that because exercise is important in both my diseases. But, it takes a while to sink into my addled brain. Because your description is exactly how I responded to gout, and it’s completely wrong.
As with allopurinol treatment for uric acid control, gout pain control has to be personal. But, it’s absolutely vital to maintain normal walking. Otherwise, you end up with posture problems. And that can lead to pains everywhere, but usually back, hips, knees, ankles, and feet.
As well as personal pain control, the biggest thing I learned was how you help your feet during a gout attack. Soft shoes and slippers seem the obvious choice. But, they give no support at all. What you need is strong shoes or boots, with layers of socks for added support.
I know it can be hard to accept this. I just summarized several years of my life experiments with gout in a few sentences. So, I have to leave now and focus on getting my new personal gout plan service fully operational. Because all your answers lie there.
Keith TaylorParticipantKeith (the site’s owner) advocates the maximum dose which would be 800mg or 900mg but I think that would be pointlessly risky in most cases.
Allopurinol Dose
I certainly advocate 900mg allopurinol per day (UK maximum) for me. But, I hope I have stressed that every gout patient must work with their doctor to maintain the correct dose for that person. Importantly, they must consider how to manage dose changes safely. So, the safe way to use allopurinol is:
1. Start with 100mg and assess effects on uric acid, kidney function, and liver function.
2. Increase allopurinol dose over a period of time to achieve target uric acid for debulking.
3. Monitor uric acid crystal debulking to assess when to move to the maintenance phase.
4. Decrease allopurinol dose over a period of time to maintain the agreed long-term safe uric acid levels.
5. Check annually and adjust dose as necessary.I should emphasize that monitoring your blood with the 3 tests at step 1 is vital throughout. Also, you have to discuss any perceptions you have about side-effects with your doctor. Most importantly, the time periods, doses, and targets are different for every gout patient.
Allopurinol Risk
Prior to starting allopurinol, I spent lots of time researching risks. Then, I reached the personal conclusion that the risks of untreated gout compared to allopurinol are an ocean compared to a teaspoon.The only downsides I found were situations where dinosaur doctors insisted on prescribing allopurinol negligently. The upsides indicated many positive advantages from long-term allopurinol use.
So, I really don’t understand “pointlessly risky in most cases”
To me, risks are only pointless when you take them without consideration. Therefore, taking ANY dose of allopurinol is a pointless risk without the detailed personal allopurinol treatment plan that I summarized in 5 core steps.
Keith TaylorParticipantNow that I can see thousands of interested visitors here, I have done some more research.
Specifically, I went looking for infectious diseases that might be related to high uric acid or gout. Because that would explain my ideas from my original post. But, the results I found don’t shine much light on the problem.
Firstly, I looked at Pyelonephritis, which is the medical term for a kidney infection. But, the research I found was not conclusive or specific. Next, I looked at HIV. But again, there is no clear link. Because the most likely gout cause is HIV treatments. Rather than the infectious disease itself.
So, it remains an interesting topic. But there is little evidence to show that secondary gout is contagious. However, there might be a small number of edge cases that I haven’t found yet.
To conclude:
1. Gout is definitely not contagious.
2. Infectious diseases might cause secondary gout. But I cannot support this with case results yet.
3. If you have septic arthritis, but you think it is gout, you might spread that disease.Keith TaylorParticipantP.S. I missed:
“I would like to request that my doctor test the fluid in the joint but I’m wondering if anyone knows how painful this is?”Get this done by the expert rheumatologist that I mentioned. Never ever get a joint fluid test from a doctor who does not have immediate test facilities. Also, check that those facilities include all appropriate tests, not just a polarizing microscope.
If fluid cannot be tested as soon as it is drawn, it is a complete waste of time.
If tests do not include all life-limiting possibilities, you put your health at serious risk.
Finally, if it is done correctly, you will not feel anything at all. Trust me, as I’ve had my ankle done by a properly trained rheumatologist. I had to ask when the test was going to start after it had already been done! But, a less qualified medic might not have the right quality of needle to ensure a painless fluid draw.
Keith TaylorParticipantSeriously, Eia, you can’t keep putting your health at risk like this. Because you clearly do not have gout. But, you might have something that requires immediate medical attention.
Treating gout is very easy for most people. But, like all diseases, it is totally dependent on getting the diagnosis right. Because there are lots of diseases that have gout-like symptoms. So, what you need is a rheumatologist who is expert in differential diagnosis.
To explain, differential diagnosis is a series of assumptions about your disease. Then tests to confirm or deny each assumption until you get the correct diagnosis. Because only then can you start to treat your ailment. Also, you need an expert to determine those life-limiting possibilities that need to be ruled out, or treated, first.
It’s good that you have taken the first step. Because you’ve assumed it is gout. Then you took the test and ruled gout out. But if you continue without expert help, this could take you a lifetime. So, I think it’s time to seek out an expert rheumatologist in your area.
As for my “recommended vegan diet”, unfortunately, I have no such thing. My approach to diet is:
Either
1) We analyze your current diet to see if we can make gout-friendly improvements. But, you don’t have gout. So, this can’t apply.
Or
2) We work on your preferences to amend your choice of Foundation Gout Diet to suit your gout. But, again it won’t work for you as you don’t have gout.My diet planning choices are because gout can only be treated with a personalized plan. And that applies to drugs, herbal, or lifestyle gout treatment. I have no idea what applies in your situation, Eia. So, I think you should eat healthy whole foods. Then take supplements that your vegan nutritionist recommends. Thus avoiding malnourishment from missing essentials.
Finally, my best recommendation would be a vegan alkaline diet. Unfortunately, I don’t know any reliable resources. For the sake of your health, use Google Scholar or PubMed if you want to research it properly. As this is not about gout, I can’t help you with that research here. And, I’ve had to put my Foodary project on hold until I get GoutPal back at the top of my game.
To conclude, I’m really sorry I can’t help you more at this time. But, if you can’t find good quality help elsewhere, you can push me to restart my nutrition project, with you first in line.
Keith TaylorParticipantGary, thanks for posting your latest results. But I hate being the bearer of bad news. Because 397 is still too high.
To explain, you don’t start gout recovery until you are down to 360. Even then, progress will be very slow. So, your target should be below 300. Then, when you have gone 6 months with no symptoms, you can relax the dose if you want.
There’s no fixed rules about how long this takes. But, we can certainly say that the more you lower uric acid, the faster the process will take.
The good news is, you have completed the first step very well. Because you have proved that allopurinol works for you. Now it’s time to go to step 2, where you increase to an effective dose. So please ask your doctor to increase allopurinol so you can get below 300.
Keith TaylorParticipantSorry Eia, I think the application form got broke. But, it should be working OK now, and I’ve included it in this reply.
However, before you apply, you should consider the issues raised by nobody, and by Rich. Because it is impossible to have gout at 3.3mg/dL, except for 2 possibilities:
Either
1) You have had uric acid much higher than 3.3 in the past. Then you need help for a short time while your body adjusts to the sudden fall in uric acid.Or
2) Your result is not 3.3mg/dL, but 0.33mmol/L. So, please check your uric acid blood test results carefully.[gravityform id=2]
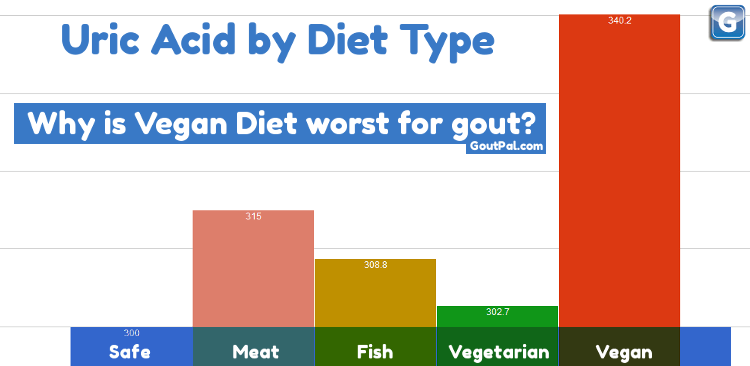
Statistics don’t make gout diets – people do!
But, statistically, vegans are most at risk of gout. See Why Vegan Diet is Worst for Gout for more information.
Keith TaylorParticipantGreat stuff, jokeco68, now I have more to go on. Then, as I get to know your situation better, we’ll get nearer to a plan that works for you.
As well as uric acid tests, I always recommend blood tests for kidney function and liver function. Because that is absolutely the best starting point for assessing and dealing with side-effects.
nobody makes lots of valid points, and the one that stands out is febuxostat. Because that could be a quick answer to the side-effects you blame on allopurinol. However, in the USA, febuxostat is overpriced Uloric and I don’t know if that affects Canadian costs.
Also, it’s absolutely essential to get liver function tests on febuxostat. Although adverse liver reactions are rare, they are too serious to risk without regular checkups. By which I mean monthly blood tests until you get uric acid stable. Then less frequent, but always at least once a year.
If febuxostat isn’t an option, we can look at better ways to manage allopurinol dose. But, I can’t see a clear timeline yet. So, was there a dose of allopurinol that worked for you without side-effects? If so, we should be able to come up with a package combining low-dose allopurinol with something else.
Finally, jokeco68, are you going to name and shame the so-called doctor who “flatly refused my request for a lab visit as he feels those readings fluctuate depending on what you eat.” Because we need to warn your fellow Canadians to stay well clear.
Keith TaylorParticipantI had an unusual allopurinol side effect, Patrick. Because allopurinol gave me all the benefits of better quality of life that you mention. But, I never expected that hidden boost in my self-confidence that came from taking control. 😀
Also, I remember a fight to get the right dose of allopurinol. Getting started was no problem. But I had to explain to 2 different doctors why 7 mg/dL is not low enough!
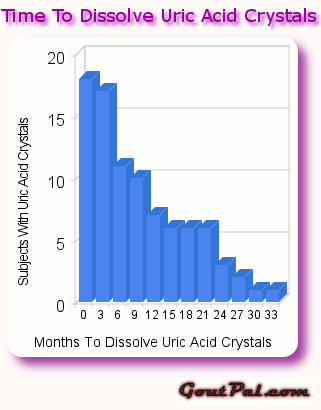
The sooner you start allopurinol, the sooner you dissolve your uric acid crystals!
Keith TaylorParticipantHi, d_q, nice to see more interesting questions.
The thing about my three-pronged gout pain attack plan is that it’s mine. Because, if there is only one thing you are ever allowed to remember about gout treatment it’s: “Treat To Individual Target”. So, my personal plan is actually at Acute Gout Attack Treatment Plan. But, there are many individual points to discuss how that would apply to anyone else.
Therefore, I don’t want to post it as a “quickly accessible thread”. Because I feel it should be a slowly ingested example of a plan. Then, other gout patients can inspect each point to see how it applies to them. Unfortunately, that’s a longwinded process. So, doctors have to rely on standards that have served them through their careers. Because sometimes you have to accept “average” treatment if there are only 10-15 minutes available.
Otherwise, nothing would ever get prescribed. But in this gout forum, we can guide patients through the process.
Firstly, we have to understand individual attitudes to pain. Because pains that might be tolerated by one person will put another in bed. This is important because, in my experience, immobility tends to extend the duration of a gout flare. But, I have not yet found science to support this in the general gout population.
Next, we consider each of the points:
1. Inhibit Inflammation.
2. Reduce Inflammation.
3. Block Residual Pain.1. Colchicine. To answer your initial question, I’d suggest one colchicine at night. Then another in the morning, as required. But, that might not fit an individual’s lifestyle. Also, there’s evidence to suggest it’s not always the most appropriate dose. So, at best it’s a starting point for a discussion between doctor and patient. Ultimately, all I’m really trying to do is support gout patients so they ask the right questions and understand their doctor’s responses.
On the other hand, colchicine might be totally inappropriate for some patients. Because it suppresses the immune system. So, depending on personal circumstances it can be a very bad idea.
2. We can see here, there are opposing views on NSAIDs and steroids. Some think that the immunosuppressive nature of drugs like methylprednisolone, methylprednisone, and corticosterone can support or replace colchicine for gout. Others, like me, would never consider them. In any case, we cannot give general guidance for specific NSAID choice or dosing. Because that’s the doctor’s job.
Anyway, all NSAIDs are medically similar. So, most doctors will just prescribe the one they are most used to. Then, if a patient doesn’t get on with it, they might try a different one. For example, ibuprofen, naproxen, and indomethacin are common choices. But even though one might seem better tolerated than another, they all have bad cardiac risks after long periods of high doses.
3. I’ve heard 2 arguments about paracetamol dosing as an addition to NSAIDs. I was taught to intersperse the dose. That is, NSAID at every 4 hours starting at zero hours. With paracetamol every 4 hours starting after 2 hours.
But a friend, whose extreme pain experiences are different from mine, recommends taking them together. “Because they work differently, so provide more pain relief when taken at the same time”. Anyway, I think this goes back to being mindful about your pain symptoms, and the effects of treatment. Then, you can adjust dosing to suit your situation.Always remember, doctors will suggest dose intervals based on average half-life and other factors. But, within drug safety limits, there is a great deal of flexibility.
To summarize, I hope you can see why doctors often prescribe a “one-size-fits-all” treatment plan. Because they simply do not have time to discuss all these different aspects. Also, in most cases, the patient gets the pain relief they want. So, it’s only worth discussing individual cases when there is a specific problem. In that case, the starting point is almost certainly different from my Acute Gout Attack Treatment Plan. And, the problems are always unique.
Finally, to answer your question “someone gets an acute flare today; what would be your dosing to hit hard?”
Dear Someone (related to nobody?),
Ask your doctor if the following is safe given your medical history:
1. Take 2 colchicine immediately (for 0.5mg or 0.6mg pills) with the maximum dose of ibuprofen. Try to keep affected joint moving.
2. At 2 hours, if symptoms persist, take another colchicine with maximum dose paracetamol (acetaminophen). Try harder to keep affected joint moving.
3. At 4-5 hours, repeat ibuprofen. Are you really trying to keep moving? Note that I’ve considered increasing the interval if symptoms are more tolerable. Sometimes I consider reducing the dose.
4. At 6-8 hours, repeat paracetamol. Accept you’re a wimp when it comes to pain tolerance.
If your doctor is concerned about any aspect of this emergency gout flare treatment, let’s discuss how we can improve it just for you.Yours with love, tolerance, and patience.
KeithI wonder if anyone kept reading long enough to read the final answer?
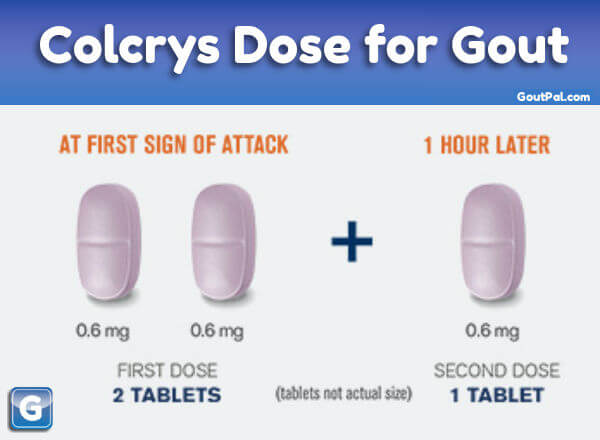
There is a standard colchicine dose for gout. But be flexible depending on your plan and your symptoms.
Keith TaylorParticipantHi jokeco68, and thanks for your kind words. I’ve just sent you a welcome email. So, you can see where to edit your Profile, if you want to change your Display Name. Or, maybe jokeco68 is your nickname??!
I’m very interested, and very patient. But, I’m also often longwinded, so I hope you are also patient.
How did I persuade you to start allopurinol without also convincing you of the need to get regular blood tests? Because without that, I cannot give you any worthwhile advice.
So, I might as well write about the placebo effect. But I’ll try to stop myself. Except to say the power of the mind accounts for one-third of all treatment benefits. And, just as it applies to positive benefits, so the power of the mind applies to negative side-effects.
Just to be clear, are you telling me you never had a blood test! I realize Canadians are a special breed. But, that’s because I thought you are especially kind and good. If you’re going to run a health service without blood tests, please explain how that works. Or, have you just forgotten to post whatever results you have?
Anyway, without information, everything is just a guess, so here are my guesses.
1. I guess allopurinol is working fine because your gout flares are getting less frequent and less severe. Also, you went a long time with no obvious side-effects. But, that just means you relax your diet, eat badly, and gain weight. Then, the extra weight puts a strain on your body. So that, coupled with poor diet causes swollen lower legs.
2. I guess the failure to stay healthy, coupled with approaching 50 years old and a complete change in sexual lifestyle give you an occasional drop in sexual performance. But, instead of dealing with the real causes, you look for excuses. Because, if you Google side-effects of any drug long enough, you will find something that fits.
So here’s my plan!
1. Fly me to Canada and give me accommodation.
2. I will supervise your eating, exercise, and waistline.
3. Then, I’ll persuade your doc that blood tests are necessary.
4. You’ll get back into shape, and gout will stop.Other personal gout support plans are available! 😉 🙂
Let me know how you want to proceed. I hope I don’t need to explain that my little plan is tongue-in-cheek. Because, seriously, we can crack this. But, we have to take it one step at a time. So my first step is to truly understand your blood test situation. Because it’s an essential part of any uric acid lowering therapy.
Your best first step is to tell me the contact details of whoever is prescribing your allopurinol. Because if they haven’t broken the law by refusing blood tests, they have broken every ethical code.
In the meantime, stop reading crap from people you don’t know about allopurinol side effects. It’s not helpful and it will make you worse.
Let’s learn about your gout together.
Keith TaylorParticipantAlso, I just read a nice summary of this situation[*].
The authors make it clear that the first-line treatment for tophi should be uric acid lowering drugs including allopurinol, febuxostat, probenecid, lesinurad, and pegloticase. However, they also note that some tophi cause “urgent complications” that might warrant surgery. Those complications include infection, ulceration, and nerve compression (e.g. carpal tunnel syndrome). Also, when tophi develop near joints, they can damage joints, restrict movement, and cause function loss.
Finally, they conclude that tophi removal by surgery is generally successful. Although they repeat the warning “surgery should be considered for the rare patient with impending or severe, debilitating complications”.
So, it’s worth repeating that anyone with tophi should be taking allopurinol, or similar, at a sufficient dose to get uric acid well below 5mg/dL. But, each patient must have dose monitored to ensure it is safe and effective for that individual.
Tophi, Surgery, Uric Acid Lowering Reference
Kasper, Isaac R., et al. “Treatment of tophaceous gout: When medication is not enough.” Seminars in arthritis and rheumatism. Vol. 45. No. 6. WB Saunders, 2016.Keith TaylorParticipantHi Gainesville Gout Sufferer,
I hope you can see from my earlier replies that your surgeon was right to be cautious. Because surgery to remove tophi is a risky procedure. But, self-mutilation, under-qualified lancing, or simple neglect are all too common. Then, without careful, sterile, tophi removal, surgical washing, and medical dressing, the risks of infection are high.
Also, burst tophi are often slow to heal. Because the damage you experience with your own tophus can affect skin healing.
However, you should search for tophus removal using the search box at the top of the page. Because the first result is Tophi Removal Without Surgery. So, that picture proves you can ‘liquefy a hard tophus’. But, only by lowering uric acid.
I’m surprised your surgeon hasn’t referred you to a rheumatologist. Because you need to get your uric acid as low as you can. Starting, as soon as you can.
If you need help with that, you can reply to this topic. But, I think it would be better if you log in and start your own new topic.
-
AuthorPosts